






I was born in 1963 which technically makes me a Baby Boomer but I certainly wasn’t experiencing the scene at Woodstock. I have referred to those born in the early 60s under a generational subset known as “Generation AIDS”. I was coming of age sexually in the early 1980s just as the AIDS crisis had cancelled the party. This crisis had a profound influence on those born in the early to mid-60s, how they saw risks and how they thought about public health issues. Harm reduction measures then were a matter of life or death.
Harm Reduction 101: The AIDS Crisis
In the early 80s, as reports of this new sexually transmitted disease were growing, there was more fear than information about the syndrome. As always, in a vacuum, prejudice and political interests proliferate. The AIDS zealots of the day, mostly conservative homophobes, imposed the abstention solution: The only way you could be safe is if you abstain from sexual relations. Soon this precautionary imposition was applied not just to sex but to saliva and touching others. I recall the shock, in 1987, six years after the crisis emerged, when Princess Diana shook hands with an AIDS patient. Bigotry, ignorance and bias ran rampant, and the media played into the fear narrative with a steady stream of celebrity diagnoses, obituaries and TV expert postulations.
As much as the health policy puritans pursued restrictive precautionary policies, seeming to almost celebrate the crisis as some divine intervention upon what they had perceived as sexual deviance, you could not expect people to abstain from casual sexual behaviour, drug use or intimate human interaction. Harm reduction measures were enacted: AIDS testing, condoms, reduced number of partners…
Without a cure or a vaccine (until today), AIDS became the largest global case study of public health harm reduction. It was not about keeping the population safe (there is no such thing as “safe”, even now as AIDS cases are still spreading) but rather creating the conditions where people could be safer in their social activities. These same people who took harm reduction measures to live through the AIDS crisis had no problem understanding how vaping or nicotine pouches could reduce the harm from smoking.
Generation AIDS and tobacco harm reduction advocates understand the difference between safe and safer.
Safe and Safer
There seems to be two lenses through which public health policy is seen: those who demand 100% safe health policies and those who work to make public health safer. In the regulatory arena, this can be translated to advocates for uncertainty management (precaution) and risk management.
- The precautionary principle claims that a substance or process can only be allowed on the market if you can prove, with certainty, that it is safe. If this burden of proof is not achieved, then precaution would be applied. Precaution takes the hazard-based approach: if some substance, practice or product is considered hazardous, it is deemed unsafe, no matter how low the exposure levels. The precautionary principle lies at the heart of EU Directives from REACH to the Sustainable Use of Pesticides Directive. This, of course, is a political tool, since any scientist would never use absolutist terms like “safe” or “certain” in research or regulatory advice.
- Scientists, like most people, use risk management tools which follow an entirely different (“risk-based”) approach. Risk equals hazard times exposure. A chemical may be a hazard, but if the exposure level is very low, then so is the risk. Risk management is the practice of reducing our exposures to hazards to as low of a level as reasonably possible. Here risk managers work toward a continuous, reasonable process of making exposures safer.
Reducing exposures is harm reduction and both are important tools in risk management.
Nothing is 100% safe and if the EU consistently applied the precautionary principle, then all products would be taken off the market. Precaution is only brought out of the policy toolbox when it pleases the regulator and when there are alternatives (on pesticides, chemicals, plastics, food additives, and now, it seems, on nicotine).
Nicotine Alternatives are 95% Safer
How does this distinction of “safe” and “safer” apply to the present tobacco harm reduction debate? Tobacco smoke is a known hazard and exposure to it is an important risk. Common sense would state that the best way to reduce exposure to this hazard is to quit smoking, and many smokers have tried, unsuccessfully. The second-best way to manage the health risks from smoking is to reduce exposure to harm via alternative nicotine products like e-cigarettes or nicotine pouches. These strategies have been determined to be 95% safer than exposure to combustible cigarette products (see image below).
Instead, the tobacco control zealots, like the AIDS abstention puritans, rejected the 95% safer argument as “still a risk”, justifying their evident illogic by playing the “children” and the “we just don’t know if it’s safe” cards to enforce their prohibitionist strategy. This confirms the Zaruk Hypothesis: If you pay activists enough, they will try to justify the most absurd claims.
The zero-risk, precautionary strategy demanding 100% safe can have serious consequences. During the COVID pandemic, most European countries quickly resorted to precautionary lockdowns, keeping populations indoors until it was safe, with no regard to the consequences of their failure to use other risk management tools. By taxing or banning alternative nicotine harm reduction products known to be far safer than smoking, what do EU regulators think will happen to the overall health of smokers?
This strategy is the opposite of risk management, as more smokers, confused by the ignorance and misinformation spread by the anti-nicotine campaigns, continue to smoke, exposing themselves to much greater hazards. To justify this horrible consequence, the mostly Bloomberg-funded activists leading the MPOWER and FCTC campaigns at the WHO claim that the very concept of harm reduction was a ruse contrived by the tobacco industry to continue to get consumers addicted to their products. (See note above about the Zaruk Hypothesis.)
Harm Reduction: A Concept Created by Big Tobacco?
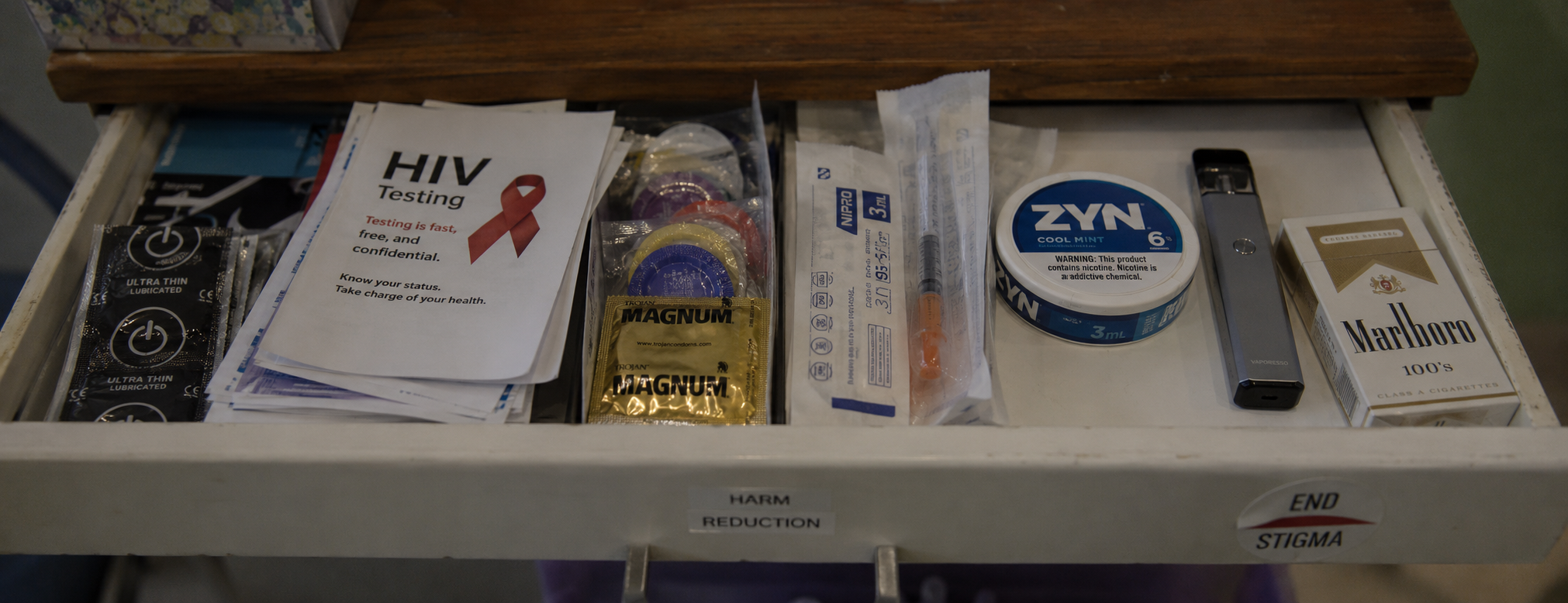
Those receiving handsome salaries paid by Michael Bloomberg (Big Bloomberg) have tried to label the term “tobacco harm reduction” as a concept created by Big Tobacco. The term “harm reduction” is widely used in public health and safety arenas, from the use of needle exchanges and methadone centres for drug users to seatbelts to sunscreens. These tobacco control activists must be much younger than me and have no idea how the AIDS crisis had interrupted Western societies. As a survivor of Generation AIDS, it is absolutely ridiculous to hear such individuals claim that the term “harm reduction” is merely a corporate slogan.
The tobacco control zealots seeking to ban alternative nicotine products share much in common with the homophobic abstinence puritans speaking out during the AIDS crisis in the early 1980s. They insist on some mythical world that is 100% safe (and reject “safer” as a strategic interference). I suspect, like the AIDS abstinence puritans from 45 years ago, the anti-nicotine prohibitionists are offended by the thought of people enjoying pleasure without consequences (thus their vindictive calls for flavour and packaging bans).
Generation AIDS survivors look down on the anti-nicotine health zealots in the same way as other zero-risk nanny state activists seeking a perfect, 100% safe world (without alcohol, sweet drinks, processed foods and liberal sexual attitudes). They are amused when these highly paid Bloomberg activists, enforcing prohibitions of pleasure while advancing their degrowth, anti-industry witch-hunts, fabricate a story of pro-vaping advocates being paid off by Big Tobacco.
With $2 billion to spend on this single campaign, Big Bloomberg has more money, but far less common sense.

